Key takeaways
- Mounjaro does not have one universal calorie target because an appropriate intake depends on individual nutritional needs, health, activity, goals, and care guidance.
- SURMOUNT-3 used approximately 1,200 calories for women and 1,500 for men during an intensive, supervised lifestyle program, not as universal Mounjaro instructions.
- Persistent fatigue, weakness, dehydration clues, or an inability to eat and drink can signal that reduced appetite needs attention from your care team.
- Protein and resistance training deserve attention during GLP-1 weight loss because an estimated 25% to 40% of lost weight may come from lean mass.
- Smaller meals, slower eating, bland foods, and fluids between meals may make eating easier when nausea or low appetite gets in the way.
Table of contents
- What calorie target should you use on Mounjaro?
- How do you know if you are eating too little on Mounjaro?
- Why does protein matter more than chasing a perfect calorie number?
- How can you eat enough when Mounjaro makes food unappealing or nauseating?
- What should you track before discussing calories with your care team?
What calorie target should you use on Mounjaro?
How many calories should I eat on Mounjaro? There's no single target. Your appropriate intake depends on your nutritional needs, health, activity, goals, symptoms, and care plan. The numbers people often quote came from supervised research protocols, not universal instructions for everyone taking the medication. In SURMOUNT-3, women were instructed to eat approximately 1,200 calories daily and men approximately 1,500, but those targets belonged to a structured 12-week lifestyle program with professional support and monitoring.
What did SURMOUNT-1 test?
SURMOUNT-1 tested more than a medication alone. Adults with obesity or overweight and at least one qualifying complication were assigned tirzepatide or placebo, with every group receiving diet and exercise support. People with type 2 diabetes were excluded, and all four groups were followed for 72 weeks. That design shows how tirzepatide performed within lifestyle support. It does not reveal one calorie target responsible for the results or suitable for every reader.
The three SURMOUNT trials answered different questions in different populations. Their lifestyle structures help explain why a calorie figure from one protocol cannot simply become everyone’s daily target.
Trial | Population | Dietary context | Duration | What it tells us | What it cannot tell us |
|---|---|---|---|---|---|
SURMOUNT-1 | Obesity or overweight; diabetes excluded | Diet and exercise support in every arm | 72 weeks | Medication performance with lifestyle support | Your ideal daily calorie intake |
SURMOUNT-2 | Obesity and type 2 diabetes | Treatment compared with placebo | 72 weeks | Results in a diabetes population | One target for different care plans |
SURMOUNT-3 | Successful intensive-intervention participants | Counseling, logs, activity, optional meal replacements | 12-week lead-in; then 72 weeks | Calories used in one supervised protocol | A universal Mounjaro calorie prescription |
Why was SURMOUNT-3 different?
SURMOUNT-3 began with an intensive 12-week lifestyle phase. Participants attended eight in-person counseling sessions with a dietitian or similarly qualified professional. The program allowed up to two portion-controlled meal replacements daily, encouraged at least 150 minutes of moderate activity weekly, and requested three-day diet and exercise logs before counseling visits. Its calorie figures were therefore one component of a closely structured intervention, not stand-alone instructions for ordinary life on Mounjaro.
- Screened participants: Each trial applied eligibility rules, so its population does not represent every body, health history, or nutritional need.
- Fixed study design: Researchers used consistent procedures to compare groups, while personal calorie discussions must account for circumstances outside that protocol.
- Qualified counseling: SURMOUNT-3 paired its targets with eight sessions led by a dietitian or similarly qualified healthcare professional.
- Exercise support: Participants were encouraged to complete structured activity, which changes the context surrounding both intake and weight outcomes.
- Population differences: SURMOUNT-1 excluded type 2 diabetes, while SURMOUNT-2 specifically studied adults who had obesity and type 2 diabetes.
- Ongoing monitoring: Diet and exercise logs gave the research team context that a calorie number by itself could never provide.
Why can appetite matter more than the number?
When Mounjaro leaves you less hungry or feeling like nothing sounds good, the useful question is not simply whether you stayed under a number. It is whether the food that still fits is meeting your needs consistently. SURMOUNT-3 asked participants to complete three-day food and exercise logs before counseling visits. That wider view captured patterns a calorie total misses, including what was eaten, how activity changed, and whether a prescribed structure remained workable over time.
A trial target standardizes research; a personal target must fit the person who will actually eat, move, and live with it.
The weight changes in these trials were substantial, but they do not identify one ideal intake. In SURMOUNT-1, mean 72-week changes were −15.0%, −19.5%, and −20.9% with 5, 10, and 15 mg tirzepatide, versus −3.1% with placebo. SURMOUNT-2 reported −12.8% and −14.7% with 10 and 15 mg, versus −3.2% with placebo. Nature Medicine reported an additional −18.4% in SURMOUNT-3 versus a 2.5% increase with placebo after its intensive lead-in. Each result reflects an entire study design, not calories alone.

A better next question is whether reduced appetite is pulling intake too low. Rather than pushing calories downward because the scale is the goal, notice whether meals repeatedly disappear, food variety narrows, fluids fall away, or normal energy becomes harder to maintain. Those patterns give your care team more useful context than a single calorie ceiling. They also shift the conversation toward adequacy: what your body is receiving, what keeps getting missed, and whether your current approach remains sustainable between appointments.
How do you know if you are eating too little on Mounjaro?
Look for a repeated pattern, not one unusually light day. Frequently missed meals, persistent fatigue or weakness, dehydration clues, or being unable to keep food and fluids down deserve more attention than an occasional low-appetite day. Reduced appetite can lower both the volume and variety of food you eat, while ongoing nausea, vomiting, or diarrhea can also cause fluid loss. Record what is happening and contact your care team promptly when stomach symptoms do not resolve or drinking becomes difficult.
Which signs deserve attention?
Less hunger is expected for many people, but an increasingly narrow eating pattern deserves a closer look. Cleveland Clinic notes that Mounjaro can reduce appetite and slow digestion. The nutrition concern begins when smaller portions repeatedly become skipped meals, or when both food quantity and variety keep shrinking. That pattern can leave nutritional gaps even if weight continues changing. A short record of meals, fluids, symptoms, and ordinary activity can help your care team assess the pattern without turning any single symptom into a diagnosis.
- Persistent fatigue: Record whether it returns after low-intake days instead of assuming one tired afternoon proves that you need more calories.
- Muscle weakness: Note changes in ordinary tasks or usual activity, particularly when your food volume has remained low for several days.
- Dry mouth or thirst: Compare these symptoms with fluid intake, hot weather, activity, and any recent nausea, vomiting, or diarrhea.
- Dark urine: Treat a repeated darker color alongside low fluid intake or stomach symptoms as useful information for your care team.
- Lightheadedness: Write down when it happens, what you recently ate or drank, and whether you take other diabetes medicines.
- Persistent stomach symptoms: Contact your care team promptly when nausea, vomiting, or diarrhea does not go away or prevents drinking.
Several of these patterns can have more than one explanation. Record the surrounding details rather than assigning the cause yourself, then use persistence and severity to decide how quickly to contact your care team.
Pattern | What else may be involved | What to record | Care-team timing |
|---|---|---|---|
Fatigue or weakness | Repeated low or narrow intake | Meals, energy, ordinary strength | ✅ Routine review if persistent |
Thirst, dry mouth, headache | Fluid shortfall or stomach symptoms | Drinks, heat, activity, symptoms | ✅ Review soon if recurring |
Dark urine or lightheadedness | Possible dehydration or fluid loss | Urine color, dizziness, fluid intake | ⚠️ Prompt contact if persistent |
Ongoing vomiting or diarrhea | Dehydration and kidney concerns | Duration, fluids kept down, urination | ⚠️ Prompt contact |
Possible low blood sugar | Insulin or sulfonylurea use | Timing, medicines, agreed glucose plan | ⚠️ Follow care-team plan promptly |
Could dehydration be part of the problem?
Thirst, dry mouth, headache, dark urine, or feeling faint can point toward dehydration. Cleveland Clinic includes those among the signs to recognize, especially when vomiting, diarrhea, heat, or activity increases fluid loss. A practice-oriented nutrition checklist uses 1.5 to 2 liters daily as a monitoring benchmark, but that is not a personalized prescription. Review what you are actually drinking and whether ongoing stomach symptoms are making fluids difficult. Contact your care team promptly when those symptoms persist or worsen.
Spontaneous restriction can become nutritionally unbalanced even while the scale keeps moving. Lower appetite and stomach symptoms may reduce both how much you eat and the range of foods that still sound tolerable. That narrower pattern can make micronutrient gaps and loss of lean body mass harder to notice from weight alone. This is why nutrition monitoring looks beyond calories to meal variety, hydration, strength, and whether you can maintain a workable eating pattern over time.
What if you also take diabetes medicines?
Do not guess whether a symptom is low blood sugar. The FDA label says people taking insulin or sulfonylureas should discuss low blood sugar and how to manage it with their care team before using Mounjaro. If lightheadedness, weakness, or another concerning symptom appears, follow the glucose-monitoring and treatment plan your care team has already given you. Keep the timing of meals, symptoms, Mounjaro, and other diabetes medicines together in your notes so the pattern can be reviewed accurately.
Review three to seven ordinary days together. Record meals and snacks, approximate fluids, nausea or bowel symptoms, energy, and anything that changed your routine. Mark days when you could not eat or drink normally, but do not let one calorie total decide the conclusion. Repeated gaps are more informative: meals skipped across several days, fluids staying low, symptoms clustering after eating, or energy falling with the same pattern. Bring that short record to your care team instead of trying to diagnose the cause from an app total.
What fits into a limited appetite matters as much as the total amount. A practice-oriented benchmark calls for at least 130 grams of carbohydrate daily, alongside attention to fluids and protein, but it is not a personal prescription. The larger point is that a low calorie total can conceal missing food groups, limited variety, or too little material for maintaining lean body mass. Once intake is consistently small, the next useful conversation is about preserving nutritional value and strength, not merely choosing a lower number.
Why does protein matter more than chasing a perfect calorie number?
Protein deserves priority when appetite is low because a smaller calorie total can also mean less of the material your body uses to maintain and repair muscle. Protein provides those building blocks, while weight loss can include lean tissue as well as fat. An estimated 25% to 40% of weight lost during GLP-1 therapy may come from lean mass, although the share varies. That does not make one protein target universal, but it does make protein distribution and muscle-supporting movement more useful to watch than a perfect calorie number alone.
What are the signs of muscle loss?
The scale cannot separate fat from lean tissue. Watch instead for a pattern: unusual muscle weakness, persistent fatigue, normal tasks feeling harder, or recovery that seems slower than usual. Slow wound healing can also be a clue that nutrition deserves review, although none of these signs proves muscle loss and other causes are possible. Their value is in showing a change from your baseline that you can describe to your care team, especially when it appears alongside very low intake.
Clue | Daily note | Compare over time | What it can reveal | Bring to your care team | Question to ask |
|---|---|---|---|---|---|
Strength changes | Loads, repetitions, grip-heavy tasks | Repeat one familiar task weekly | A decline from your baseline | Persistent weakness or lost capacity | Is this change persistent? |
Routine activity | Stairs, walks, groceries, household tasks | Rate effort, not only completion | Whether normal tasks feel harder | Changes affecting daily function | Could intake or recovery matter? |
Protein distribution | Protein source at each meal or snack | Mark long gaps between eating | Whether protein clusters in one meal | What fits when appetite is low | Does my daily target fit? |
Healing | Cuts, bruises, recovery after activity | Note changes from your normal | Whether healing seems slower | Slow wound healing | Should nutrition be reviewed? |
Overall intake | Meals, snacks, fluids, food variety | Review several days together | Repeatedly low volume or variety | Patterns, not one light day | Am I meeting nutrient needs? |
Should you use current or goal weight for protein?
Use the calculation as a conversation starter, not a prescription. The published method converts pounds to kilograms by dividing by 2.2, then multiplies kilograms by a grams-per-kilogram target. It does not settle whether your current weight, goal weight, or another clinical reference point should anchor the math, and that choice can change the result. Ask your care team or a registered dietitian which weight basis fits your health, body composition, activity, and goals before treating the result as your daily target.
For active weight loss, the cited range is 1.2 to 1.6 grams per kilogram per day. It is a framework, not a one-size-fits-all instruction. Individual needs may vary with age, kidney health, activity, and other health factors, so the appropriate target requires personal guidance. If you have kidney concerns or a condition that affects nutrition, bring the range to your care team before changing your intake or adding a supplement. The goal is a usable target that fits your care plan, not the biggest number.
How can you prioritize protein when nothing sounds good?
When nothing sounds good, start with protein. Mayo Clinic suggests eating it first so it is less likely to be left on the plate, then spreading protein sources across the day. Smaller portions can feel more realistic than one protein-heavy meal. You can also add protein without much extra bulk, such as Greek yogurt or powder in a smoothie, cottage cheese with vegetables, or beans in soup. This is where protein needs on a GLP-1 can become more practical than one large daily goal.
- Greek yogurt: Choose a small serving on its own, or stir it into foods when a larger plate feels like too much.
- Protein smoothie: Blend a modest portion with protein powder or Greek yogurt for a softer option that adds protein without much bulk.
- Protein shake: Keep the serving small and sip slowly when chewing a full meal feels unappealing or difficult to finish.
- Soup: Choose a simple soup that feels easy to tolerate, then add a protein source rather than relying on broth alone.
- Vegetables with cottage cheese: Pair a small amount of vegetables with cottage cheese for protein without turning the snack into a large meal.
- Beans in soup: Stir beans into a favorite soup to raise protein and nutrient density without adding a separate side dish.
Lowering calories changes the total. Preserving the protein that still fits protects the nutritional value of what you eat.
What role does resistance training play?
Resistance training works alongside protein to support muscle during weight loss. A common framework is two to three sessions per week using bodyweight, bands, or weights, but individual ability and health matter. Start slowly if the work is new, and check with your care team when health conditions affect exercise. Mayo Clinic describes a gradual path from wall-supported movements to harder bodyweight versions, then greater load or difficulty over time. Bodyweight work can count at the beginning, so progress does not require forcing a specific exercise or pace.

Related reading
- How GLP-1 medications reduce appetite
- Real GLP-1 weight-loss timelines
- How long tirzepatide takes to work
- Protein needs on a GLP-1
- Combining GLP-1 treatment with exercise
- Why GLP-1 medications can cause nausea
How can you eat enough when Mounjaro makes food unappealing or nauseating?
Make eating smaller and easier, not perfect. Mayo Clinic recommends smaller, more frequent meals, a slower pace, cool bland foods, and water or ginger tea between meals for nausea. Those adjustments may make it easier to keep some food and fluid coming in when nothing sounds good. Avoid forcing a large plate to meet a number. Build several modest eating opportunities instead, using foods you can tolerate. If intake keeps shrinking despite these changes, the repeated pattern matters more than one light meal or one low day.
How should you structure meals to reduce nausea?
Meal structure can address several common trouble spots at once. Keep portions small and the pace slow. Mayo Clinic advises against skipping meals, high-fat or fried foods, strong odors, and lying down after eating when nausea is active. Cool foods such as crackers, toast, or pretzels may be easier to try. These are tolerance strategies, not a requirement to eat a particular menu. Use the combination that helps you maintain regular small meals and fluids without turning each eating time into a large task that day.
- Eat smaller meals: Divide the day into several modest eating opportunities so one large plate does not become the only chance to eat.
- Avoid skipping meals: Keep a simple eating rhythm even when hunger is quiet, using a small tolerated option instead of waiting for strong hunger.
- Choose cool, bland foods: Try crackers, toast, or pretzels when hot foods or strong smells make eating feel less appealing.
- Limit rich or fried foods: Set aside high-fat meals while nausea is active, since Mayo Clinic lists them among foods to avoid.
- Eat slowly: Take a calmer pace and pause between bites, giving a small portion time before deciding whether more will sit well.
- Sip between meals: Keep water or ginger herbal tea nearby and drink regularly through the day rather than concentrating fluids at mealtime.

What if nausea keeps returning?
Mild symptoms may begin easing within days to weeks as your body adjusts, according to Mayo Clinic, but recurrence still deserves context. Contact your care team promptly if nausea or vomiting is severe, symptoms last for several days, or you cannot eat or drink. Those are not situations to solve by lowering calories further or waiting for another meal adjustment to work. Note when the pattern began, whether fluids stay down, and what you have managed to eat so the conversation starts with specifics from the past day.
How can this fit into daily life?
Your shot does not have to match a meal. The FDA label allows Mounjaro once weekly at any time of day, with or without food. During travel, Mayo Clinic advises keeping meal times as close as practical to your usual routine. For nausea, fresh air and staying upright after eating are simple adjustments from Mayo Clinic’s guidance. That lets you separate the shot schedule from the eating strategy: keep the prescribed schedule, then arrange small meals and fluids around what you can tolerate.
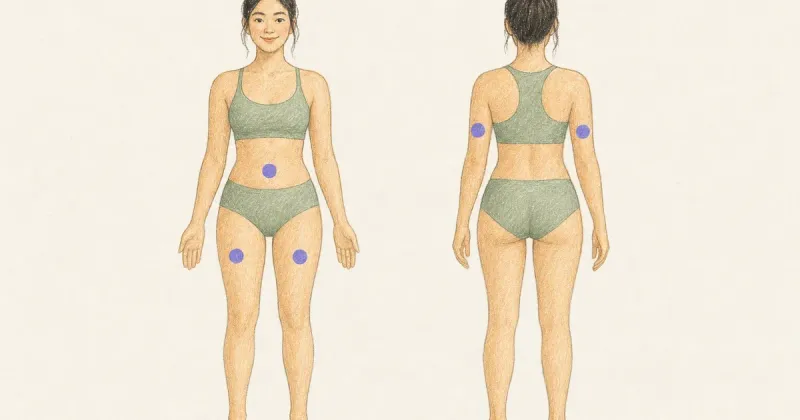
Where can Mounjaro be injected?
The labeled shot areas are the abdomen and thigh. For the back of the upper arm, the April 2026 FDA label says another person should give the injection. Rotate injection sites with each dose rather than returning to exactly the same spot. Your care team should show you how to prepare and inject your prescribed Mounjaro presentation before the first use. If the area or technique is unclear, ask for another demonstration instead of guessing through an unfamiliar step on your own.
Preparation starts with technique training for your exact presentation. The FDA label instructs patients and caregivers to be trained before use. It also says to inspect Mounjaro visually: the solution should be clear and colorless to slightly yellow. Do not use it if you see particles or discoloration. Because packaging can differ, follow the Instructions for Use that came with your prescription and ask your care team to confirm any step that does not match what you were shown before your next dose.
Safe handling depends on the presentation you use. The FDA Instructions for Use say people using vials should use a new syringe and needle for every injection, and a Mounjaro KwikPen must never be shared, even if the needle is changed. If you also use insulin, the label allows injections in the same body region but says they should not be adjacent or mixed. Ask your care team or pharmacist which instructions apply to your supplies before changing any part of your routine at home.
Once the day-to-day fixes are in place, track the pattern across the week. Note what and how much you could eat, which fluids stayed down, when nausea appeared, and whether smaller meals or bland foods helped. Add your shot day and injection area so the timing is clear without making a causal conclusion. A few specific days give your care team more context than a vague memory of feeling off. The next step is to look for recurrence, not to assign yourself a calorie prescription.
What should you track before discussing calories with your care team?
Bring a pattern, not a single calorie total. A useful conversation starts with several consecutive days of meals, fluids, symptoms, energy, strength, activity, shot details, and weight context. Note what you actually managed to eat, including days when nothing sounds good, rather than trying to make every entry look ideal. The goal is to show your care team how intake changes across real life. That wider view supports an individualized nutrition discussion and makes it easier to ask whether your current approach fits your health, goals, diabetes plan, and daily schedule.
What belongs in a daily log?
Record quantity and variety together. If reduced appetite or stomach symptoms change what feels manageable, list the foods and portions you could eat, not just a calorie estimate. A day built from one narrow set of foods may look different from a day with varied eating opportunities. The 2025 Nutritional and Lifestyle Supportive Care consensus statement treats nutrition, body composition, physical activity, and common stomach symptoms as connected parts of GLP-1 supportive care. Your daily log becomes a compact record of what happened, when it happened, and what else changed.
- Meals and protein: Record each meal or snack, rough portions, what you ate first, and whether protein appeared across several eating opportunities throughout the day.
- Fluids: Note drinks and approximate amounts, plus any long gaps when a busy schedule, low appetite, or stomach symptoms made drinking less manageable.
- Stomach symptoms: Log nausea, vomiting, diarrhea, or constipation, including when each symptom began, how bothersome it felt, and whether it affected eating or drinking.
- Energy and strength: Record fatigue, changes in ordinary tasks, planned activity, and anything that felt noticeably easier or harder than it normally does.
- Shot and trend: Note shot day, your prescribed dose, weekly weight, and any clear shift in appetite, symptoms, strength, or normal activity afterward.

What patterns matter across a week?
Repetition matters more than one odd day. Scan the week for clusters: meals repeatedly missed, the same limited foods showing up, fluids dropping, stomach symptoms intensifying, energy fading, or ordinary tasks feeling harder. Then check timing. Did the pattern gather around shot day, travel, a busy shift, or another change you recorded? The consensus statement emphasizes considering nutrition, body composition, physical activity, and stomach symptoms together, while acknowledging limited direct evidence. Treat the log as a way to spot a pattern worth discussing, not as a tool for diagnosing its cause.
This is where MeAgain can make the week visible. Log meals, drinks, symptoms, energy, activity, shot day, prescribed dose, and weight as they happen. At the end of the week, look across the entries rather than judging any single day. You may notice that intake is repeatedly thinner after shot day, that protein appears only once on low-appetite days, or that nausea and fatigue travel together. Bring those observations to your care team as concrete examples. The log supplies timing and context without turning an app total into a calorie prescription.
When should you consult a dietitian or care team?
Book an individualized review when the pattern keeps repeating or your questions need more than a generic calorie rule. Bring forward repeated gaps in food variety, symptoms that keep bothering you, changes in strength or usual activity, and questions about a diabetes meal plan. Mayo Clinic advises regular progress checks and following the meal plan supplied by your care team for diabetes care. The 2025 consensus also notes that direct evidence for nutrition support with GLP-1-based therapies remains limited. A dietitian or care team can assess the whole picture, including your health history, instead of assigning a target from the log alone.
The scale raises a question. It does not answer it. A weight-loss stall calls for context, not a verdict.
Start with the timeline. Put several weeks of weight entries beside meals, fluids, symptoms, strength, activity, shot details, travel, and other routine changes. Look for a shift that happened before the stall, but do not assume that two events appearing together proves one caused the other. The consensus statement acknowledges that direct nutrition evidence for GLP-1-based therapies remains limited. Use the full pattern to form better questions: Has food variety narrowed? Are symptoms interrupting meals? Has normal activity changed? The purpose is to guide an individualized review, not to diagnose under-eating from the scale alone.
A routine nutrition appointment fits questions about calorie frameworks, meal composition, recurring gaps, or maintaining strength. Contact your care team promptly when stomach symptoms are severe, continue, or repeatedly interfere with eating and drinking. If you cannot keep food or fluids down, do not wait for the next routine appointment. If you have diabetes and are concerned about low blood sugar, follow the monitoring and response plan your care team gave you rather than trying to infer the cause from hunger, fatigue, or the calorie log alone.
Bring specific questions, not a request for one magic number. Ask what calorie framework fits your health, activity, goals, and current eating pattern. Ask whether current weight, goal weight, or another reference should guide your protein discussion. Find out whether your symptoms, limited food variety, or strength changes warrant laboratory testing or a dietitian referral. If the same symptoms recur around shot day, ask how your nutrition approach can adapt without changing your prescription on your own. A concise weekly record gives your care team the context needed to answer those questions individually and decide what deserves follow-up.
Related reading
- Managing GLP-1 acid reflux
- How much water to drink on a GLP-1
- Dehydration and kidney-stone risk
- GLP-1 side effects women may notice
- Tracking food while taking a GLP-1
- Tracking side effects and spotting patterns
- Tracking progress beyond the scale
- What counts as a GLP-1 plateau
- How many weeks without weight loss count as a plateau
- Weight changes after stopping a GLP-1
Frequently Asked Questions
Do I need to count calories every day while taking Mounjaro?
Not necessarily. An individualized nutrition discussion needs context, and calorie totals are only one part of that context. A short, consistent record of meals, fluids, symptoms, energy, activity, shot details, and weight may show more than a precise number entered on one unusual day. Ask your care team how much detail is useful for your goals and health needs. Ultimately, how many calories should I eat on Mounjaro is a question best answered with your care team over time, not from a single day's count.
Should I use my current weight or goal weight to calculate protein needs?
There is no single weight basis that fits everyone. The available consensus acknowledges limited direct evidence for nutrition care with GLP-1-based therapies. Bring both numbers to your care team or dietitian and ask which reference fits your health, activity, body-composition goals, and current eating pattern. Avoid treating an online calculation as a personal prescription.
Can eating too little make Mounjaro weight loss appear to stall?
A stall alone cannot establish its cause. Review several weeks of meals, food variety, fluids, symptoms, strength, activity, shot details, and weight history together. That record may identify questions worth raising, but timing alone does not prove that low intake caused the change. Use the pattern to support an individualized care-team discussion rather than lowering calories further based on the scale.
Do I need to eat before taking my Mounjaro shot?
No meal is required by the FDA prescribing information. Mounjaro can be administered with or without meals. Follow the schedule and technique provided with your prescription, and ask your care team whether your usual meal timing should change because of recurring symptoms or your diabetes plan.
What should I do if nausea keeps returning even after I switch to smaller meals?
Contact your care team if nausea continues or remains bothersome. Mayo Clinic notes that a health professional may suggest ways to prevent or reduce side effects. Seek prompt guidance if nausea repeatedly interferes with eating or drinking, becomes severe, or comes with vomiting that prevents you from keeping food or fluids down. Bring your symptom and meal log so the pattern is easier to assess.
This article is for informational purposes only and is not medical advice. Always talk to your doctor or care team about your medication, symptoms, or treatment plan.
