
GLP-1 medications have gained attention for their weight-loss effects, but rising costs and supply shortages have led many to consider alternatives. Compounded weight loss medication has emerged as a lower-cost option, though questions about safety, effectiveness, and legitimacy naturally arise. Understanding what these pharmacy-compounded versions actually are and whether they meet the same standards as brand-name medications becomes crucial for making informed decisions.
Finding reliable information about compounded semaglutide and tirzepatide can feel overwhelming when weighing health options. Licensed healthcare providers can evaluate individual situations and help patients understand the benefits and risks of compounded medications versus FDA-approved alternatives. MeAgain's GLP-1 app offers clear guidance on both compounded options and traditional prescriptions.
Table of Contents
- What Is Compounded Weight Loss Medication and How Does It Work?
- Why Compounded Weight Loss Medications Exist (And Why They’re Often Misunderstood)
- Compounded vs Approved Weight Loss Medications: Differences in Results, Safety, and Consistency
- When Compounded Weight Loss Medication Makes Sense (And When It Does Not)
- No Matter Which Medication You Choose, This Is What Determines Your Results
Summary
- Compounded weight loss medications emerged as a legal workaround during FDA-declared drug shortages, not as permanent alternatives to brand-name products. Federal law permits compounding pharmacies to prepare versions of patented medications only when commercial supply cannot meet patient demand. The semaglutide shortage that began in 2022 left patients scrambling for continuity, creating the opening for compounded versions. That legal window opened specifically because patients needed access, not because compounders offered equivalent products at lower prices.
- Compounded medications face no bioequivalence requirements despite containing the same active ingredients as FDA-approved drugs. Generic drugs must prove through pharmacokinetic studies that they enter your bloodstream at the same rate and concentration as brand-name versions. Compounded semaglutide and tirzepatide skip that entire testing framework. The pharmacy preparing your medication determines which inactive ingredients are used, how the formulation is mixed, and which quality protocols apply, with oversight standards varying significantly across states because 503(A) compounding pharmacies are regulated by state boards, not the FDA.
- Ingredient sourcing in compounded weight loss medications raises serious safety questions that FDA-approved products never face. Some pharmacies use semaglutide salts (such as semaglutide acetate) instead of semaglutide base, which differs chemically from the form in Ozempic and Wegovy. Research published in the Journal of the Endocrine Society found this substitution matters because semaglutide salts may behave differently in your body, potentially affecting both efficacy and safety profiles. Other facilities purchase ingredients from non-FDA-registered suppliers or use chemicals labeled "for research use only," meaning those substances were never intended for human consumption.
- Alternative delivery methods for compounded GLP-1s lack the clinical validation that injectable formulations underwent. Compounded semaglutide is available as sublingual drops, orally disintegrating tablets, and nasal sprays, yet no FDA-approved versions of these delivery methods exist because no manufacturer has demonstrated they work. Absorption rates through nasal membranes or under your tongue differ dramatically from subcutaneous injection. Without studies measuring blood levels and clinical outcomes, patients hope the pharmacy's formulation delivers enough active drug to produce results, but no data confirm that assumption.
- Cost barriers justify compounding only after exhausting manufacturer savings programs, insurance appeals, and alternative dosing schedules. Northwestern University obesity experts note that 42% of U.S. adults have obesity, yet many face monthly costs exceeding $1,000 for brand-name GLP-1 medications without insurance coverage. Choosing compounded versions purely to save money while FDA-approved products remain accessible through existing coverage traded off documented safety and efficacy for unvalidated consistency, accepting unknown risks from ingredient variability, potency uncertainty, and sterility questions.
- Daily nutrition and movement habits determine weight loss outcomes far more than medication choice, yet most patients treat these factors as secondary concerns. When you eat 800 calories daily because GLP-1s suppress hunger, your body breaks down muscle tissue for energy rather than selectively burning fat, slowing your metabolism and leaving you weaker than when you started. You need roughly 0.8 to 1.0 grams of protein per pound of goal body weight daily to preserve lean tissue, plus adequate fiber to prevent severe constipation and water intake to reduce nausea and fatigue.
- MeAgain's GLP-1 app addresses this by turning protein, fiber, water, and movement targets into daily check-ins that keep you consistent through the weeks when motivation fades but medication adherence still requires showing up.
What Is Compounded Weight Loss Medication and How Does It Work?
Compounded weight loss medication refers to custom-prepared versions of drugs (often GLP-1 receptor agonists like semaglutide or tirzepatide) made by licensed pharmacies when standard options are unavailable or unsuitable for a patient's needs. The FDA defines pharmacy compounding as "combining, mixing, or changing ingredients to create a customized medication for an individual patient based on a licensed practitioner's prescription." While these medications use FDA-approved ingredients, the compounded product itself has not undergone FDA review for safety, effectiveness, or quality before reaching patients.
"Combining, mixing, or changing ingredients to create a customized medication for an individual patient based on a licensed practitioner's prescription." — FDA Definition of Pharmacy Compounding

How GLP-1 medications work in your body
The active ingredients in these medications (semaglutide and tirzepatide) are glucagon-like peptide-1 (GLP-1) receptor agonists that mimic a hormone your gut naturally produces after eating. When injected, they bind to GLP-1 receptors throughout your body, triggering biological responses that reduce appetite and promote weight loss. Your brain receives stronger satiety signals, making you feel full sooner and stay satisfied longer between meals. The medication also slows gastric emptying (the rate at which food leaves your stomach), extending fullness and reducing the urge to eat again quickly. These combined effects create a caloric deficit without the constant hunger that undermines most traditional diets.
What does compounding actually change about the medication?
When a pharmacy compounds these medications, it adjusts dosage strengths to levels not sold commercially (such as 0.15 mg weekly instead of the standard 0.25 mg starting dose) or changes the delivery method. Compounded semaglutide may appear as sublingual drops, orally disintegrating tablets, oral capsules, nasal sprays, or traditional injections drawn from vials rather than pre-filled pens. A patient allergic to a preservative in Wegovy's formulation, for example, could receive compounded semaglutide injections with that allergen removed while keeping the same active ingredient.
Why doesn't the same active ingredient mean the same product?
The critical distinction: same active ingredient does not equal same product. Generic drugs must prove bioequivalence to their brand-name counterparts through rigorous FDA testing, demonstrating identical absorption rates and concentrations. Compounded medications face no such requirement.
A compounded semaglutide injection may contain the same active molecule as Wegovy, but without bioequivalence testing, there's no guarantee your body will absorb it the same way or that you'll experience the same therapeutic effects. The FDA announced in February 2025 that the semaglutide shortage had ended, yet compounded versions continue circulating. Tirzepatide remains compounded due to ongoing legal disputes, despite its shortage ending earlier.
What legitimate medical needs does compounding address?
Compounding meets medical needs that store-bought products cannot. Patients who have trouble swallowing pills can receive liquid versions instead. Those requiring micro-dose adjustments between standard strengths (stepping down from 1.0 mg to 0.75 mg weekly to manage side effects) can obtain the precise dosage they need.
Local pharmacies have different compounding capabilities, so medications requiring customization are typically sent to outsourcing facilities that specialize in preparing these formulations at scale. These outsourcing pharmacies operate independently from brand-name manufacturers (Novo Nordisk for semaglutide, Eli Lilly for tirzepatide), creating versions designed to replicate the originals during FDA-declared shortages.
When does cost alone not justify compounding?
Cost alone doesn't justify compounding when FDA-approved products remain available. The law permits copying patented medications only during official shortages, and making minor changes to circumvent FDA requirements violates those regulations.
If you've been using compounded semaglutide, you may need to switch to Ozempic or Wegovy now that supplies have stabilized. Rybelsus (oral semaglutide for Type 2 diabetes) remained available throughout shortages, and as of January 2026, Wegovy (semaglutide) entered the market as an FDA-approved option.
How do pricing models affect compounded medication value?
When deciding if compounded medications work for you, clear pricing and good support systems are as important as the medication itself. Platforms like MeAgain's GLP-1 app charge for the app subscription rather than adding extra costs to the medication, so your price remains stable even as your dosage increases, unlike many competitors.
That no-extra-cost model combined with dose tracking, nutrition guidance, and progress monitoring transforms how you think about compounded medications. Rather than viewing them as a cheaper option, you can see them as part of a comprehensive care system designed to keep costs predictable as you build sustainable habits throughout your weight-loss journey.
Related Reading
Why Compounded Weight Loss Medications Exist (And Why They’re Often Misunderstood)
Compounded weight loss medications are often mistaken for cheaper copies of drugs like Ozempic or Wegovy. Compounded GLP-1s emerged to address FDA rules during drug shortages when regular supply couldn't meet patient demand, not as counterfeit versions designed to cost less.

"Compounding fills a critical gap when FDA-approved medications are unavailable due to manufacturing shortages or supply chain disruptions." — FDA Guidance on Drug Shortages

How did drug shortages create the opening for compounded versions?
The semaglutide shortage that began in 2022 left patients struggling to maintain their medication supply. Novo Nordisk's manufacturing capacity could not meet demand driven by off-label weight loss use and social media visibility. According to Northwestern University obesity experts, 42% of U.S. adults have obesity, creating significant pressure on limited supplies.
During shortages, federal law allows compounding pharmacies to prepare versions of patented medications they would otherwise be prohibited from copying. That legal window opened because patients needed access, not because compounders offered a permanent alternative.
Why is the shortage justification legally critical?
Tirzepatide followed a similar path. When Mounjaro and Zepbound couldn't meet demand, compounding facilities stepped in using the same active pharmaceutical ingredient from overseas suppliers. The shortage justification is legally critical: it's the only reason these compounded versions can exist while the original drugs remain under patent protection.
Remove the shortage, and the legal basis for compounding disappears.
Why do people assume compounded and FDA-approved medications are equivalent?
People focus on price and assume lower cost means only the brand name is removed, treating compounded semaglutide like store-brand ibuprofen. FDA-approved generic drugs must demonstrate bioequivalence through studies showing that the medication reaches the bloodstream at the same rate and to the same extent as the brand-name version.
Compounded medications don't have this requirement because they're not classified as generics and don't undergo FDA approval.
How does regulatory oversight differ for compounded medications?
503(A) Compounding pharmacies are regulated by state boards of pharmacy, not the FDA. This means oversight standards vary significantly across states. Some facilities pursue voluntary accreditation to demonstrate quality standards, though not all do.
The pharmacy that prepares your compounded semaglutide determines which inactive ingredients are used, how the medication is mixed, what cleanliness protocols apply during preparation, and what quality testing (if any) occurs before the vial reaches you.
When does medical need justify compounding risks?
Compounding meets medical needs that store-bought products cannot. A patient allergic to a preservative in Wegovy's formula needs that ingredient removed. Someone who experiences severe nausea at standard starting doses might benefit from a lower strength (0.15 mg weekly instead of 0.25 mg). Patients with needle anxiety might prefer sublingual drops or oral tablets, though these delivery methods lack the testing rigor of injections.
How can you avoid cost-driven compounding decisions?
These scenarios represent real customization, not cost arbitrage. The problem arises when compounding becomes the default option solely because it's cheaper, even though FDA-approved products remain available and the patient has no medical need that those products cannot meet.
When weighing compounded medications against FDA-approved alternatives, pricing transparency matters. Platforms like MeAgain's GLP-1 app separate medication costs from care delivery by charging for the app subscription rather than marking up prescriptions, so your price stays stable as your dosage increases. The app's zero-markup model, paired with dose tracking and nutrition guidance, positions compounded medications within a structured care system where predictable costs support long-term adherence.
But knowing why compounded medications exist doesn't answer whether they work as well as the drugs they're designed to replace.
Related Reading
Compounded vs Approved Weight Loss Medications: Differences in Results, Safety, and Consistency
The differences between compounded and FDA-approved weight loss medications show up in how carefully they're tested, how ingredients are checked, how they're made, and what proof exists that what you inject works the way it should. When you choose between these options, you're deciding how much risk you're okay with taking in order to get the medication more easily.
Factor | FDA-Approved | Compounded |
|---|---|---|
Clinical Testing | ✅ Extensive trials | ❌ Limited testing |
Quality Control | ✅ Strict oversight | ❌ Variable standards |
Ingredient Verification | ✅ Guaranteed purity | ❌ Inconsistent verification |
Manufacturing Standards | ✅ FDA-regulated facilities | ❌ Pharmacy-based mixing |
Efficacy Proof | ✅ Clinical data required | ❌ Theoretical effectiveness |
Safety Monitoring | ✅ Ongoing surveillance | ❌ Limited tracking |
How do FDA-approved medications ensure safety?
Ozempic, Wegovy, and Rybelsus underwent years of clinical trials involving thousands of people before reaching pharmacies. The FDA inspected manufacturing facilities, reviewed safety data across diverse populations, and verified that each dose delivers consistent levels of semaglutide. This approval process establishes a clear record linking the medication to specific health outcomes documented in controlled studies.
What oversight do compounded versions receive?
Compounded semaglutide bypasses that framework. Pharmacies obtain active pharmaceutical ingredients, combine them with inactive components, and produce finished medications without submitting safety or efficacy data to federal regulators. The FDA does not review these formulations before patients receive them. You're trusting that the compounding pharmacy followed proper protocols, used pharmaceutical-grade ingredients, and produced a sterile product, but no external agency verified those assumptions.
What ingredients are used in commercial versus compounded semaglutide?
Commercial semaglutide products use formulas refined through extensive research to improve efficacy, stability, and tolerability. The inactive ingredients (preservatives, buffers, stabilizers) have been tested alongside the active drug to ensure they don't interfere with semaglutide metabolism or cause unexpected reactions.
Compounded versions are based on commercial formulas but often use different inactive ingredients at the pharmacy's discretion. Some add vitamin B12, amino acids, or other supplements and market these as improved versions. These additions haven't been studied with semaglutide in clinical trials, so you're taking part in an uncontrolled experiment with unknown absorption or interaction risks.
What concerns has the FDA raised about compounded ingredient sourcing?
The FDA found serious problems with how compounded weight loss medications source their ingredients. Some pharmacies use semaglutide salts (such as semaglutide acetate) instead of semaglutide base, which is chemically distinct from Ozempic and Wegovy. According to research published in the Journal of the Endocrine Society (volume 9, issue 8, 2025), this substitution may alter the drug's efficacy and safety profile.
Other facilities buy semaglutide from FDA-unapproved suppliers, raising questions about purity and contamination, or obtain ingredients labeled "for research use only"—chemicals never intended for human consumption and that fail to meet pharmaceutical manufacturing standards.
Medication delivery and storage
Ozempic and Wegovy come as prefilled pens that deliver exact doses with each injection. Compounded semaglutide comes in multi-dose vials requiring manual drawing with a syringe, which can introduce dosing inconsistencies. Drawing 0.5 mL versus 0.52 mL results in unpredictable outcomes over weeks of treatment.
Commercial products include detailed information showing how well they work under specific temperature conditions. Compounded versions often lack this documentation, leaving uncertainty about whether the medication remains effective through its expiration date.
How do FDA-approved doses compare to custom options?
FDA-approved semaglutide products come in standardized doses tested and validated through clinical trials: 0.25 mg, 0.5 mg, 1.0 mg, 1.7 mg, and 2.4 mg weekly for Wegovy. Researchers systematically tested these doses, measuring weight loss and side-effect profiles, and identifying optimal titration schedules across thousands of patients. Your doctor's prescription is based on evidence showing what happens at that specific dose.
What are the risks of microdosing approaches?
Compounded pharmacies can create any strength, including "microdoses" far below FDA-approved starting points. Some providers promote 0.1 mg or 0.15 mg weekly as gentler entry points with fewer side effects, though no clinical trials have tested whether those ultra-low doses produce meaningful weight loss or simply delay reaching therapeutic levels.
Staying at microdoses indefinitely may minimize nausea while minimizing results, leaving you paying for medication that never delivers the outcomes the standard protocol would provide.
How do pricing models affect your treatment costs?
Pricing models matter as much as clinical evidence. Platforms like MeAgain's GLP-1 app separate medication costs from care delivery by charging for the app subscription rather than marking up prescriptions, keeping your monthly expense predictable as your dose increases from 0.5 mg to 2.4 mg.
That approach, paired with dose tracking and nutrition coaching, transforms how you think about compounded medications. They become part of a transparent care system where you know exactly what you're paying for and why.
What dosage forms are available?
Ozempic and Wegovy are injections, while Rybelsus and the Wegovy pill are oral tablets. Each delivery method underwent specific studies to demonstrate efficacy. These studies measured how quickly semaglutide enters the bloodstream, how long it remains active, and what blood concentration levels correlate with weight loss. That pharmacokinetic data doesn't transfer across delivery methods. Injectable semaglutide's efficacy doesn't guarantee sublingual drops or nasal sprays will produce identical effects.
Why haven't alternative forms been FDA-approved?
Compounded semaglutide comes in forms that have never been tested on people: sublingual drops, oral tablets, and nasal sprays. No FDA-approved versions exist because no manufacturer has proven they work. Your body absorbs the drug through nasal membranes or sublingual tissue differently than through subcutaneous injection. Without studies measuring bioavailability and clinical outcomes, you have no proof that the pharmacy's version contains sufficient active drug to be effective.
Understanding these differences leaves the hardest question unanswered: when does choosing compounded medication make sense, and when does it introduce unnecessary risk?
When Compounded Weight Loss Medication Makes Sense (And When It Does Not)
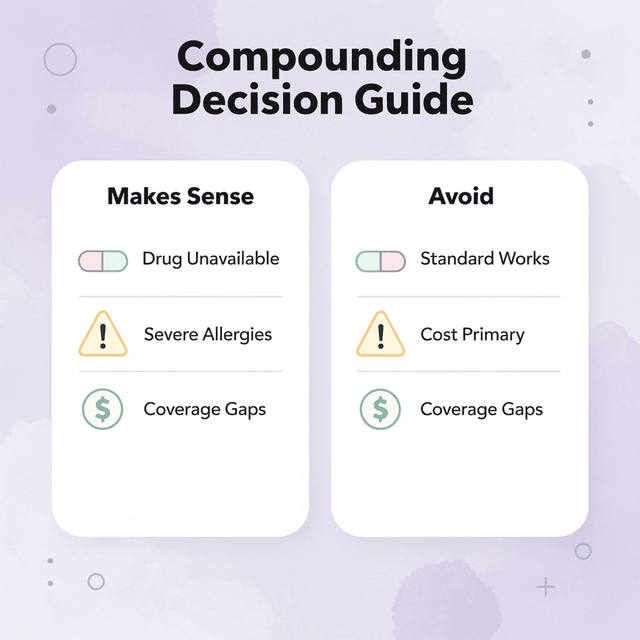
Compounded weight loss medication is not a substitute for approved drugs—it circumvents specific limits. Start with a clear question: Does an FDA-approved product meet your medical needs and fit your budget? If yes, compounding adds risk without adding value.

"Compounding should only be considered when FDA-approved medications don't meet specific patient needs or accessibility requirements." — Clinical Pharmacy Guidelines, 2024
When Compounding Makes Sense | When It Does NOT Make Sense |
|---|---|
The FDA drug is unavailable in the needed dose | Standard doses work fine |
Severe allergies to inactive ingredients | Cost savings as primary reason |
Insurance coverage gaps for approved drugs | Convenience over safety |
Specific medical conditions requiring customization | General weight loss goals |

When do compounded medications make medical sense?
Compounded medications help patients facing barriers to FDA-approved options. When Wegovy or Zepbound are unavailable despite official shortage fixes, compounded versions allow people to continue their established treatment. Abrupt GLP-1 therapy discontinuation causes rapid weight gain and metabolic complications, making temporary compounded access medically sound while approved alternatives become available.
Some patients need dosage strengths that commercial products don't offer—for example, 0.75 mg weekly to manage side effects during titration when standard options jump from 0.5 mg to 1.0 mg. Others need formulation changes because they have documented allergies to preservatives or inactive ingredients in brand-name products.
How do cost barriers justify compounded alternatives?
Cost barriers create the most common justification, but only when FDA-approved medications genuinely exceed what you can afford despite exploring manufacturer savings programs, insurance appeals, and alternative dosing schedules. According to Northwestern University obesity experts, 42% of U.S. adults have obesity, yet many face monthly costs exceeding $1,000 for brand-name GLP-1 medications without insurance coverage.
When approved options remain financially inaccessible after exhausting assistance programs, compounded versions become the only path to treatment. Your doctor should document why standard products don't work for your specific situation before prescribing compounded alternatives.
What pricing transparency should you expect?
When cost drives your decision, pricing transparency determines whether you're saving money. Platforms like MeAgain's GLP-1 app separate medication costs from care delivery by charging for the app subscription rather than marking up prescriptions, keeping your monthly expense predictable even as your dose increases from 0.5 mg to 2.4 mg, the point where many telehealth providers double or triple their fees.
That zero-markup approach, paired with dose tracking and nutrition coaching, positions compounded medications as part of a transparent care system where you know exactly what you're paying for.
When does compounded semaglutide not make sense?
Compounding makes no sense when FDA-approved medications remain accessible and affordable through your insurance or manufacturer programs. Choosing compounded semaglutide to save £200 monthly while Wegovy sits covered on your formulary trades documented safety and efficacy for unvalidated consistency.
You're accepting unknown risks—ingredient variability, potency uncertainty, sterility questions—to avoid costs you could manage through existing coverage. If your treatment requires predictable, consistent results, such as managing diabetes alongside obesity or preparing for surgery with specific weight loss targets, FDA-approved products provide the reliability that compounded versions cannot guarantee. Dosing precision matters when your A1C levels or surgical clearance depend on hitting specific therapeutic thresholds.
What risks come with unsupervised compounded medication use?
Using compounded medications without a doctor's supervision introduces a risk that far exceeds any savings. Some online providers prescribe compounded GLP-1s after brief questionnaires, without examining your medical history, monitoring your response, or adjusting treatment based on side effects or lab results.
You're self-medicating with a powerful hormone analog that affects multiple body systems, hoping your ordered dose works without causing complications the prescriber never screened for.
Choosing the right medication gets you halfway there. What you do after the injection determines whether the scale reading changes.
No Matter Which Medication You Choose, This Is What Determines Your Results
The medication you choose matters far less than what you do while it's working. GLP-1s suppress appetite and slow digestion, but they don't protect muscle mass, prevent nutrient deficiencies, or stop constipation from becoming severe. Those outcomes depend entirely on whether you hit adequate protein, fiber, water, and movement targets daily while the medication reduces your hunger signals.

Most people starting semaglutide or tirzepatide focus exclusively on the injection schedule and dosage titration, treating nutrition and activity as secondary concerns. This approach creates conditions for the worst side effects and the poorest outcomes. When you eat 800 calories daily because you're not hungry, your body breaks down muscle tissue for energy, slows your metabolism, and leaves you weaker than when you started. The medication works as designed, but your results suffer because the daily habits protecting those results never became consistent.
"When you eat 800 calories daily because you're not hungry, your body breaks down muscle tissue for energy, slows your metabolism, and leaves you weaker than when you started."
Protein intake determines whether weight loss comes from fat or muscle. You need roughly 0.8 to 1.0 grams per pound of goal body weight daily to preserve lean tissue, but GLP-1 medications make hitting that target difficult when you're not hungry. Fiber prevents severe constipation, as your gut slows significantly without adequate roughage. Water intake matters because dehydration amplifies nausea, headaches, and fatigue. Movement (even 20 minutes daily) signals your body to maintain muscle rather than break it down for energy.
Essential Daily Target | Why It Matters | GLP-1 Challenge |
|---|---|---|
Protein (0.8-1.0g per lb) | Preserves muscle mass during weight loss | Reduced appetite makes hitting targets difficult |
Fiber (25-35g daily) | Prevents severe constipation | Gut motility slows significantly |
Water (64+ oz daily) | Reduces nausea, headaches, fatigue | Dehydration amplifies side effects |
Movement (20+ min daily) | Signals the body to maintain muscle | Low energy can reduce activity levels |
Structured tracking makes the difference between guessing and knowing whether you're protecting your results. Our MeAgain GLP-1 app turns protein, fiber, water, and movement targets into simple daily check-ins guided by your capybara companion, so you're not mentally calculating macros or wondering whether you drank enough water hours ago. The Journey Card captures your progress visually as changes happen, making it easier to see what's working without obsessing over the scale. This combination of habit tracking and progress documentation keeps you consistent through weeks when motivation fades.
Download MeAgain, set your daily targets based on your current weight and goals, and track your progress on your first day. The medication creates the conditions for weight loss. What you eat, drink, and do each day determines whether those conditions produce sustainable results.
